Central Nervous System data
Central Nervous System Data
DELSTRIGO® (Doravirine/Lamivudine/tenofovir disoproxil fumarate)
Prescribing Information (United Kingdom) [External link]
PIFELTRO® (doravirine)
Prescribing Information (United Kingdom) [External link]
Doravirine/3TC/TDF = DELSTRIGO (doravirine/lamivudine/tenofovir disoproxil fumarate).
PIFELTRO® (doravirine) 100 mg film-coated tablet is indicated, in combination with other antiretroviral medicinal products, for the treatment of adults, and adolescents aged 12 years and older, weighing at least 35 kg, infected with HIV-1, without past or present evidence of resistance to the NNRTI class.
DELSTRIGO® (100 mg doravirine/300 mg lamivudine/300 mg tenofovir disoproxil fumarate, equivalent to 245 mg tenofovir disoproxil) is indicated for the treatment of adults infected with HIV-1 without past or present evidence of resistance to the NNRTI class, lamivudine or tenofovir.
DELSTRIGO® is also indicated for the treatment of adolescents aged 12 years and older weighing at least 35 kg, who are infected with HIV-1, without past or present evidence of resistance to the NNRTI class, lamivudine, or tenofovir and who have experienced toxicities which preclude the use of other regimens that do not contain tenofovir disoproxil.
Please consult the SmPC for further information before making any prescribing decisions.

DRIVE-AHEAD is a Phase 3, double-blinded, non-inferiority trial. Antiretroviral treatment-naïve adults (≥18 years) with ≥1000 HIV-1 RNA copies/mL were randomised (1:1) to once-daily, fixed-dose DOR at 100 mg, lamivudine at 300 mg, and tenofovir disoproxil fumarate (TDF) at 300 mg (DOR/3TC/TDF) or to efavirenz at 600 mg, emtricitabine at 200 mg, and TDF at 300 mg (EFV/FTC/TDF) for 96 weeks.2
The primary efficacy endpoint was the proportion of participants with <50 HIV-1 RNA copies/mL at week 48 (Food and Drug Administration snapshot approach; non-inferiority margin -10%). Of the 734 participants randomised, 728 were treated (364 per group) and included in the analyses.4
DRIVE-FORWARD is a randomised, controlled, double-blinded, multicentre, non-inferiority trial. Antiretroviral treatment-naïve adults (≥18 years) with ≥1000 HIV-1 RNA copies/mL were randomised (1:1) to once-daily DOR at 100 mg, or darunavir 800 mg plus ritonavir 100 mg (DRV/r) once daily with two investigator-selected NRTIs (tenofovir and emtricitabine, or abacavir and lamivudine) for up to 96 weeks.3
The primary efficacy endpoint was the proportion of participants with <50 HIV-1 RNA copies/mL at week 48 (Food and Drug Administration snapshot approach; non-inferiority margin -10%). Of the 769 participants randomised, 766 were treated (383 per group) and included in the analyses.5
Upon completing the double-blind phase of DRIVE-AHEAD2 or DRIVE-FORWARD3, eligible participants in both the comparator groups could switch to the study-specific doravirine-based regimen for 96 weeks in an open-label study extension. 269 participants in DRIVE-AHEAD switched from their original double-blind regimen (EFV/FTC/TDF) to open-label DOR/3TC/TDF and 233 participants in DRIVE-FORWARD switched from their original double-blind regimen (DRV/r + 2NRTIs) to open-label DOR + 2NRTIs. 1
*Participants who completed the base study (Week 48) but did not continue to extension-1 (up to Week 144) were excluded from the efficacy analysis after week 48.
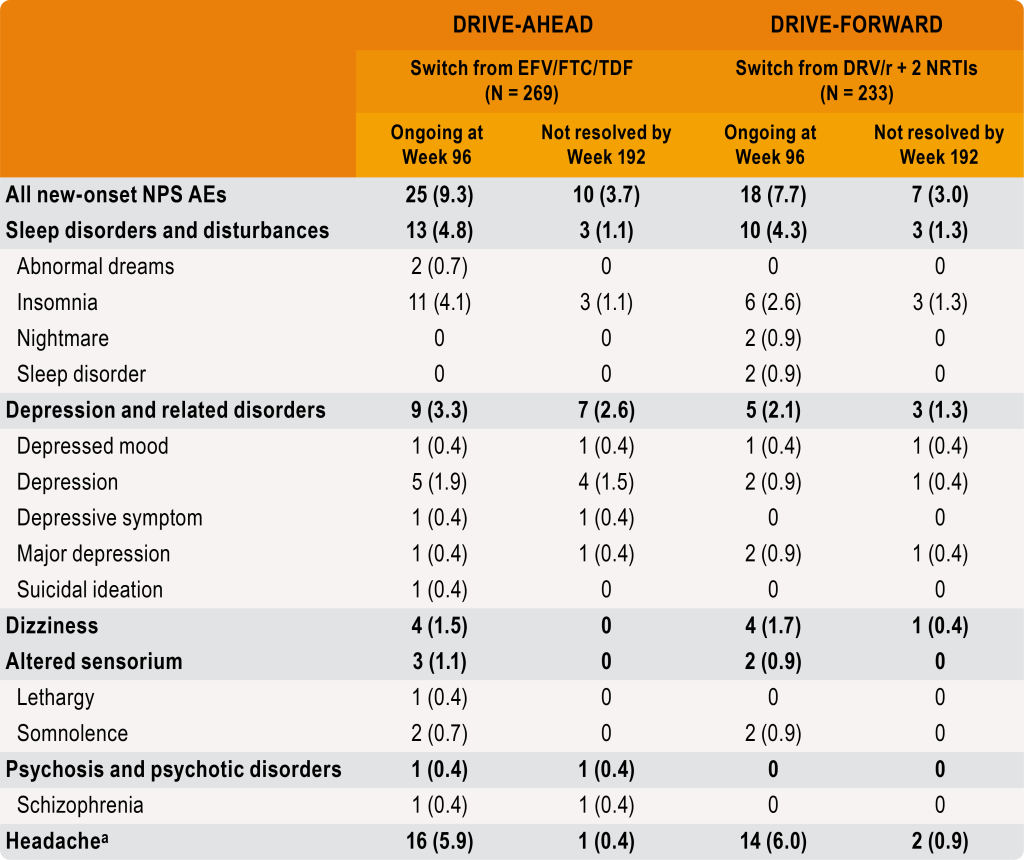
The analysis included 5 predefined categories of neuropsychiatric AEs: sleep disorders; depression and related disorders (suicide/self injury); dizziness; altered sensorium and psychoses/psychotic disorders.1 Headache was not included in the predefined NPS AE categories and is not included in the total number of participants with persisting NPS AEs.
Study design of DRIVE-AHEAD and DRIVE-FORWARD
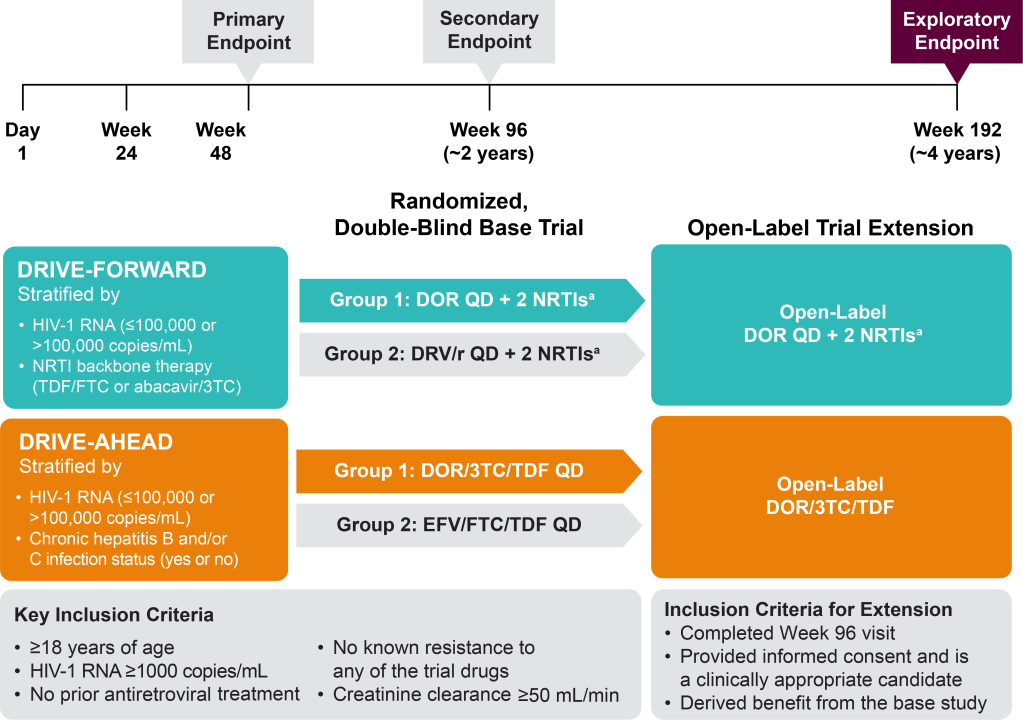
Adapted from Moyle G et al, JAIDS 2025
aNRTIs were TDF/FTC or ABC/3TC.

Key conclusions at Week 192:1
1. Persistence of neuropsychiatric AEs in the open-label extension:
Overall, neuropsychiatric AEs that occurred during the double-blind phase (Week 0–Week 96) persisted in only 3% (EFV/FTC/TDF) to 4% (DRV/r +2 NRTIs) of participants at 2 years after switching to a doravirine regimen at Week 96.
2. Resolution of ongoing neuropsychiatric AEs in the open-label extension:
73.1% of participants (19/26) with ongoing neuropsychiatric AEs at Week 96 while receiving EFV/FTC/TDF experienced resolution after switching to DOR/3TC/TDF.

Adapted from Moyle G et al, JAIDS 2025
The 5 categories of NPS AE were predefined. Specific terms included for each category were based on MedDRA 23.0. A participant with multiple AEs within a category is counted a single time for that category.
aHeadache was not included in the predefined NPS AE categories and is not included in the total number of participants with persisting NPS AEs.
Data shown as n (%).
3. Incidence of new neuropsychiatric AEs in the open-label extension:
Incidence of new neuropsychiatric AEs with doravirine regimen was lower during the open-label study extension (table 2) compared to that during the double-blind base trial (table 3).
Specific terms included for each category were based on MedDRA 23.0. A participant with multiple AEs within a category is counted a single time for that category.
aHeadache was not included in the predefined NPS AE categories and is not included in the total number of participants with new onset NPS AEs.
Data shown as n (%).
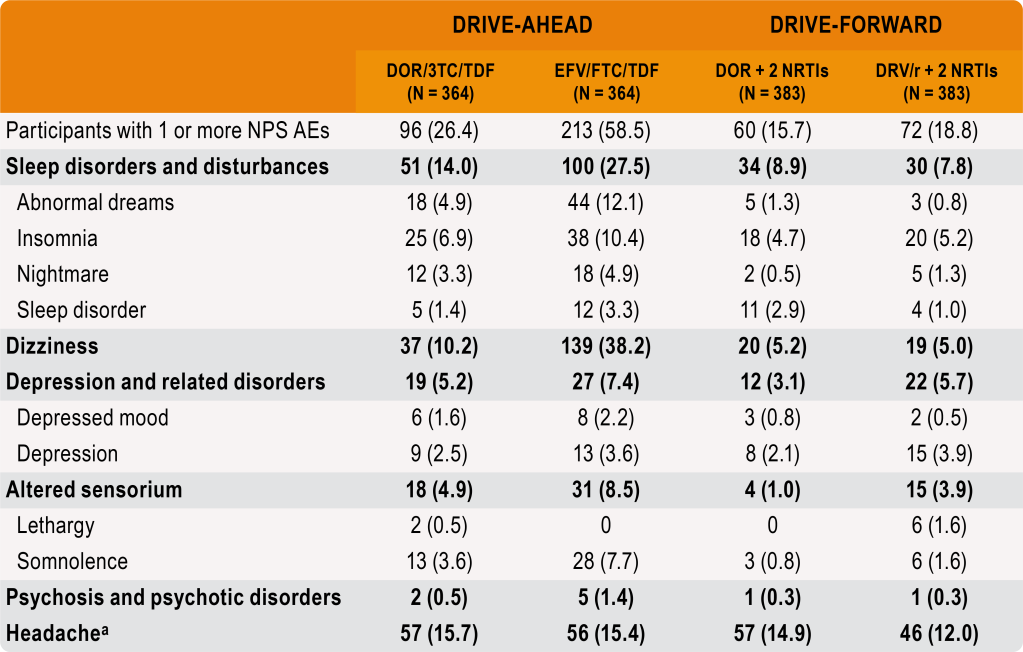
The 5 categories of NPS AE (shown in bold text) were predefined. Specific terms included for each category were based on MedDRA 20.0. A participant with multiple AEs within a category is counted a single time for that category.
Doravirine 100 mg QD and darunavir 800 mg + ritonavir 100 mg QD were administered with FTC/TDF or ABC/3TC.
aHeadache was not included in the predefined NPS AE categories and is not included in the total number of participants with 1 or more NPS AEs.
Data shown as n (%).
4. Rate of neuropsychiatric AEs with doravirine and darunavir-based regimens:
The similar rate of neuropsychiatric AEs with doravirine and darunavir-based regimens may represent the generalised background rate for these events.
Abbreviations
3TC = Lamivudine; ABC = Abacavir; AE = Adverse Event; DOR = Doravirine; DRV/r = Ritonavir-boosted Darunavir; EFV = Efavirenz; FTC = Emtricitabine; NPS = Neuropsychiatric; NRTI = Nucleoside Reverse Transcriptase Inhibitor; NNRTI = Non-Nucleoside Reverse Transcriptase Inhibitor; SmPC = Summary of Product Characteristics; QD = Once Daily; TDF = Tenofovir Disoproxil Fumarate.
References
- Graeme Moyle et al. Resolution of neuropsychiatric adverse events after switching to a doravirine-based regimen in the open-label extensions of the DRIVE-AHEAD and DRIVE-FORWARD trials. G.Moyle et al, Journal of Aquired Immune Deficiency Syndromes.( JAIDS), 2025,10.1097
- Orkin C et al. Doravirine/lamivudine/tenofovir disoproxil fumarate (TDF) versus efavirenz/emtricitabine/TDF in treatment-naïve adults with Human Immunodeficiency Virus type 1 infection: week 96 results of the randomised, double blind, phase 3 DRIVE-AHEAD non-inferiority. Clinical Infectious Disease. 2020: 1–10.
- Molina JM et al. Doravirine versus ritonavir-boosted darunavir in antiretroviral-naïve adults with HIV-1 (DRIVE-FORWARD): 96 week results of a randomised, double-blind, non-inferiority, phase 3 trial. Lancet HIV. 2020;7:16–26.
- Orkin C, Squires KE, Molina JM, et al.; and DRIVE-AHEAD Study Group. Doravirine/lamivudine/ tenofovir disoproxil fumarate is non-inferior to efavirenz/emtricitabine/tenofovir disoproxil fumarate in treatment-naive adults with human immunodeficiency virus–1 infection: week 48 results of the DRIVE-AHEAD trial. Clinical Infectious Disease. 2019;68(4):535–544.
- Molina JM, Squires K, Sax PE, et al.; for the DRIVE-FORWARD Study Group. Doravirine versus ritonavir-boosted darunavir in antiretroviral-naive adults with HIV-1 (DRIVE-FORWARD): 48-week results of a randomised, double-blind, phase 3, non-inferiority trial. Lancet HIV. 2018;5(5): e211–e220. doi:10.1016/S2352-3018(18)30021-3. Epub. 2018 March 25.
Supporting documentation
DELSTRIGO® Prescribing Information (United Kingdom) [External link]
PIFELTRO® Prescribing Information (United Kingdom) [External link]
By clicking the links above you will leave the MSD Connect website and be taken to the emc website
