KEYNOTE-189: KEYTRUDA plus chemotherapy in non-squamous mNSCLC
Prescribing Information (Great Britain) & Prescribing Information (Northern Ireland) [External links]
Discover the 5-year update from KEYNOTE-189: KEYTRUDA plus chemotherapy in non-squamous mNSCLC*
KEYNOTE-189 study design1
A randomised, multicentre, double-blind, active-controlled, phase 3 trial in patients (n=616) with previously untreated metastatic non-squamous NSCLC with no EGFR or ALK positive mutations.1
616 patients were randomly assigned (in a 2:1 ratio) to receive pemetrexed and a platinum-based drug plus either 200 mg of pembrolizumab (n=410) or placebo every 3 weeks for 4 cycles (n=210), followed by placebo or pembrolizumab for up to a total of 35 cycles plus pemetrexed maintenance therapy.1
Overall Survival and Progression-Free Survival were primary endpoints. Secondary endpoints consisted of Overall Response Rate, Duration of Response, and Safety.1
The results of this phase 3 trial were first published with a median follow up of 10.5 months.1 The latest follow up was published with a median follow up of 64.6 months.2
The original analysis1
KEYTRUDA plus chemotherapy (pemetrexed and platinum) provides superior survival vs. plat-pem for the first-line treatment of metastatic non-squamous NSCLC in adults with no EGFR/ALK positive mutations:1
- Superior OS with a 51% reduction in the risk of death (HR 0.49, p<0.001)
- Superior PFS with a 48% reduction in the risk of progression or death (HR 0.52, p<0.001)
- Survival benefit observed in each of the PD-L1 subgroups including the <1% and 1-49% expressers‡
- Superior ORR (47.6% vs 18.9%, p<0.001) and improved DOR
- A generally manageable tolerability profile. The frequency of adverse events for the combination was observed to be higher than for each agent alone, reflecting the contributions of each agent.1,3
*Exploratory endpoints – no statistical conclusions can be drawn from them.
At a median follow-up of 64.6 months, KEYTRUDA plus chemotherapy (pemetrexed and platinum) continued to provide long-term survival benefit vs. pemetrexed and platinum for the first-line treatment of metastatic non-squamous NSCLC in adults with no EGFR/ALK positive mutations:2
5 Year OS rate
19.4%
KEYTRUDA + plat/pem
vs.
11.3%
Plat/pem
(HR 0.60, p not tested)
Exploratory endpoints – no statistical conclusions can be drawn from them
Median OS more than doubled numerically
22 months
KEYTRUDA + plat/pem
vs.
10.6 months
Plat/pem
(p not tested)
Exploratory endpoints – no statistical conclusions can be drawn from them
Survival benefit observed in each of the PD-L1 TPS subgroups, including the PD-L1 TPS <1% expressers:
23.3%
KEYTRUDA + plat/pem
vs.
5.3%
Plat/pem
(HR 0.52, p not tested)
Exploratory endpoints – no statistical conclusions can be drawn from them
Median DOR at the time of updated analysis:
12.7 months
(range: 1.1+ to 68.3+)
KEYTRUDA + plat/pem
vs.
7.1 months
(range: 2.4 to 31.5)
plat/pem
(p not tested)
Exploratory endpoints – no statistical conclusions can be drawn from them
Overall Survival (OS): KEYTRUDA + plat/pem vs. plat/pem alone regardless of PD-L1 expression4,a
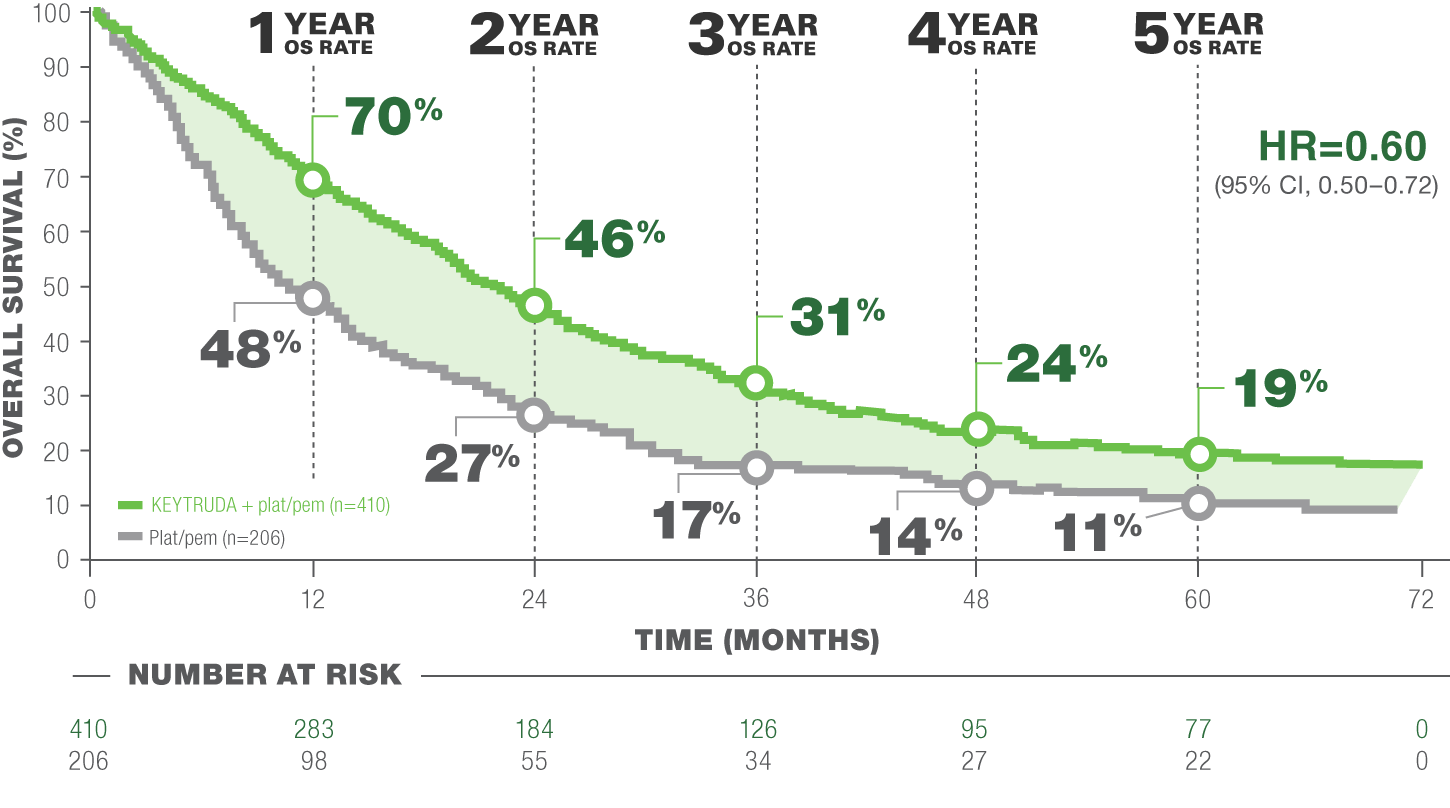
LIMITATION: This post hoc analysis (median follow-up time: 64.6 months) in KEYNOTE-189 was exploratory in nature and occurred after the protocol-specified final analysis. No formal statistical testing was planned for this analysis and, therefore, no statistical conclusions can be drawn. Trial participants in either study arm could receive subsequent anti-cancer therapy.4
CROSSOVER RATE: 57.3% of patients (118/206) crossed over from plat/pem to anti–PD-(L)1 therapy on (n=84) or off (n=34) study4,a,b
Median OS: 22.0 months (95% CI, 19.5–24.5) with KEYTRUDA + plat/pem vs. 10.6 months (95% CI, 8.7–13.6) with plat/pem alone4
Events: 80.2% (329/410) with KEYTRUDA + plat/pem and 88.8% (183/206) with plat/pem alone4
a Some patients received >1 subsequent anti-PD-(L)1 therapy.3,b
b anti-PD-L1 or anti-PD-1.
Adapted from “5-year update from KEYNOTE-189” Garassino MC, Gadgeel S, Speranza G, et al.
Summary of AEs in the as-treated population (5-year update)4
Median follow up: 64.6 months
A generally manageable tolerability profile. The frequency of adverse events for combination was comparable to previous studies. An increase in the frequency of Immune-mediated AEs and infusion reactions was observed in patients who received 35 cycles of KEYTRUDA.1-3
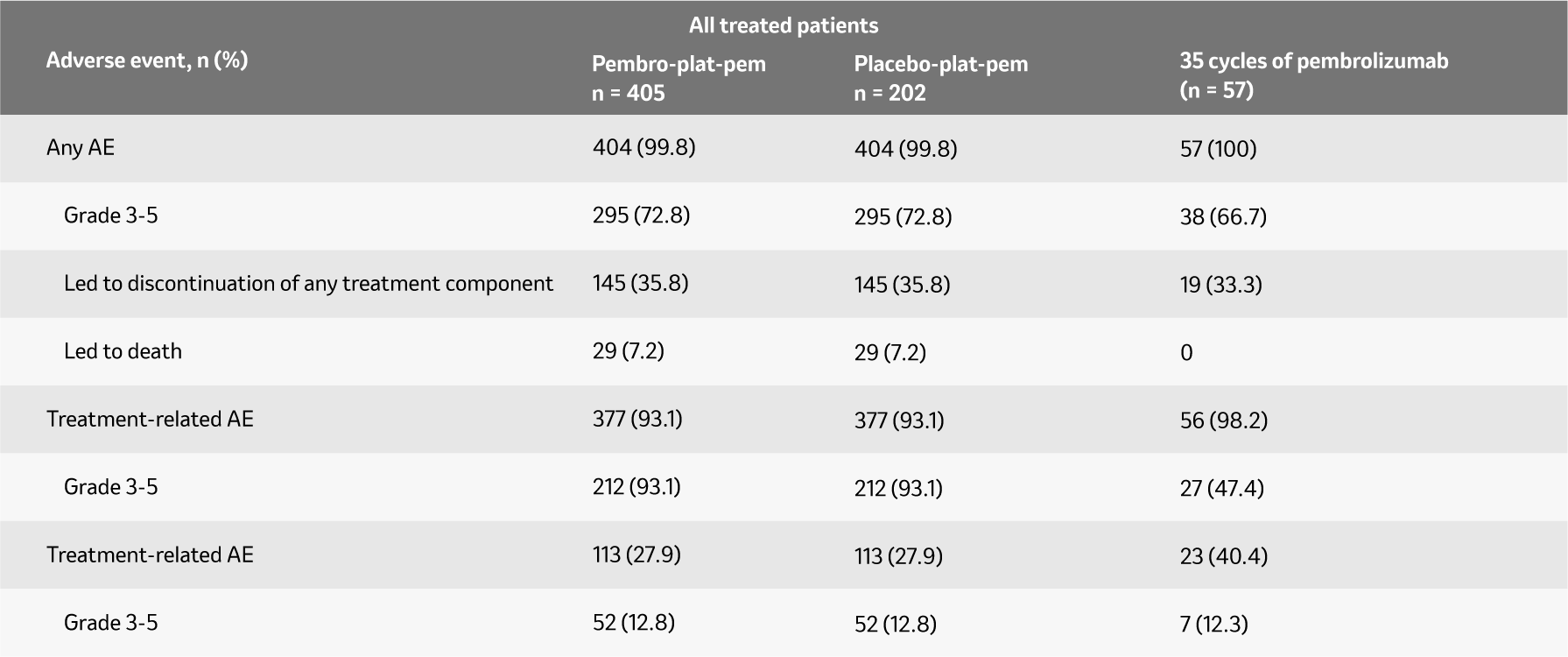
Adapted from Garassino MC et al. ESMO 2022.
Data cutoff date: March 8, 2022
a All deaths were previously reported in Rodriguez-Abreu D et al. Ann Oncol 2021,32:881-895.
b Events considered regardless of attribution to treatment or immune relatedness by the investigator.
The recommended dose of KEYTRUDA as part of combination therapy is either 200 mg every 3 weeks or 400 mg every 6 weeks administered intravenously over 30 minutes. KEYTRUDA should be administered first when given in combination with chemotherapy.3
Explore our related resources
Pembrolizumab, with pemetrexed and platinum chemotherapy, is recommended as an option for untreated, metastatic, non-squamous non-small-cell lung cancer (NSCLC) in adults whose tumours have no epidermal growth factor receptor (EGFR)- or anaplastic lymphoma kinase (ALK)- positive mutations, only if pembrolizumab is stopped at 2 years of uninterrupted treatment or earlier if the disease progresses, and the company provides pembrolizumab according to the commercial arrangement.5
Pembrolizumab is accepted for restricted use within NHS Scotland in combination with pemetrexed and platinum chemotherapy, for the first-line treatment of metastatic non-squamous non-small-cell lung carcinoma (NSCLC) in adults whose tumours have no EGFR or ALK positive mutations and whose tumours express programmed death ligand 1 (PD-L1) with a <50% tumour proportion score (TPS), or in those whom it has not been possible to evaluate PD-L1 TPS.6
KEYTRUDA, in combination with pemetrexed and platinum chemotherapy, is indicated for the first‑line treatment of metastatic non-squamous NSCLC in adults whose tumours have no EGFR or ALK positive mutations.3
The recommended dose of KEYTRUDA as part of combination therapy is 200 mg Q3W administered intravenously over 30 minutes. KEYTRUDA should be administered first when given in combination with chemotherapy.3
Find out more about KEYTRUDA in mNSCLC
KEYTRUDA in combination with Chemotherapy in non-squamous mNSCLC
Monotherapy in mNSCLC
Patient Management
Sign up to MSD emails
✔ Get the latest product updates
✔ Receive cancer resources
✔ Be the first to hear about our events
Abbreviations
carbo + pac/nab-pac = Carboplatin + Paclitaxel or Nab-Paclitaxel; CI = Confidence Interval; DOR = Duration Of Response; HR = Hazard Ratio; mNSCLC = Metastatic Non–Small Cell Lung Carcinoma; NA = Not Available; ORR = Overall Response Rate; OS = Overall Survival; PD-L1 = Programmed Death Ligand 1; PFS = Progression Free Survival; TPS = Tumor Proportion Score; Q3W = Every Three Weeks; Q6W = Every Six Weeks
References
- Gandhi L, et al. N Engl J Med. 2018: 378: 2078-2092.
- Gray JE, et al. Presented at the 2020 World Conference on Lung Cancer (WCLC), January 28–31, 2021.
- KEYTRUDA Summary of Product Characteristics.
- Garassino MC, Gadgeel S, Speranza G, et al. KEYNOTE-189 5-year update: first-line pembrolizumab + pemetrexed and platinum vs placebo + pemetrexed and platinum for metastatic nonsquamous NSCLC. Slide deck presented at: European Society for Medical Oncology (ESMO) European Lung Cancer Virtual Congress (ELCC); 9–13 September 2022; Paris, France.
- National Institute for Health and Care Excellence (2021). Final appraisal determination: Pembrolizumab with pemetrexed and platinum-based chemotherapy for untreated non-small-cell lung cancer (CDF Review of TA557) [ID1584] Available from: https://www.nice.org.uk/guidance/indevelopment/gid-ta10529. NICE guidance is prepared for the National Health Service in England, and is subject to regular review and may be updated or withdrawn. NICE has not checked the user of its content in this document to confirm that it accurately reflects the NICE publication from which it is taken
- Scottish Medicines Consortium (2019). Appraisal determination: Pembrolizumab 25mg/mL concentrate for solution for infusion and 50mg powder for concentrate for solution for infusion (KEYTRUDA®). Available from: https://www.scottishmedicines.org.uk/medicines-advice/pembrolizumab-keytruda-resub-smc2207/.
Supporting documentation
Prescribing Information (Great Britain) & Prescribing Information (Northern Ireland)
By clicking the links above you will leave the MSD Connect website and be taken to the emc PI portal website
