PIFELTRO® (doravirine) 100 mg film-coated tablet is indicated, in combination with other antiretroviral medicinal products, for the treatment of adults, and adolescents aged 12 years and older, weighing at least 35 kg, infected with HIV-1, without past or present evidence of resistance to the NNRTI class.
DELSTRIGO® (100 mg doravirine/300 mg lamivudine/300 mg tenofovir disoproxil fumarate, equivalent to 245 mg tenofovir disoproxil) is indicated for the treatment of adults infected with HIV-1 without past or present evidence of resistance to the NNRTI class, lamivudine or tenofovir.
DELSTRIGO® is also indicated for the treatment of adolescents aged 12 years and older weighing at least 35 kg, who are infected with HIV-1, without the past or present evidence of resistance to the NNRTI class, lamivudine, or tenofovir and who have experienced toxicities which preclude the use of other regimens that do not contain tenofovir disoproxil.
Please consult the SmPC for further information before making any prescribing decisions.
Metabolic Syndrome
Metabolic syndrome is a clustering of metabolic abnormalities that include visceral adiposity (increased waist circumference), insulin resistance/high blood glucose levels, increased triglycerides (TG), low high-density lipoprotein cholesterol (HDLC) and hypertension.1,2
Obesity/excess adiposity1
Dyslipidemia1
Hypertension1
Insulin resistance1
Why does it matter?
Metabolic abnormalities are known to predict increased risk of cardiovascular disease (CVD)3 and in the UK, data suggests, the incidence of CVD is higher in People Living with HIV compared with those not living with HIV4
As people living with HIV, with access to care, are ageing, age related non-AIDs co-morbidities, including CVS and metabolic disorders, increasingly account for morbidity and mortality3
Even though the benefits of ART outweigh treatment-associated risks, it is important to note the differential impact of select classes and agents on metabolic events3
What is the cardiometabolic data for doravirine?
Doravirine: Fasting Lipids Data
Improvements in All Pre-specified Lipid Endpoints vs. EFV/FTC/TDF9 and DRV/r.10
DRIVE-AHEAD is a Phase 3, double-blinded, non-inferiority trial. Antiretroviral treatment-naïve adults (≥18 years) with ≥1000 HIV-1 RNA copies/mL were randomised (1:1) to once-daily, fixed-dose DOR at 100 mg, lamivudine at 300 mg, and tenofovir disoproxil fumarate (TDF) at 300 mg (DOR/3TC/TDF) or to efavirenz at 600 mg, emtricitabine at 200 mg, and TDF at 300 mg (EFV/FTC/TDF) for 96 weeks.6
The primary efficacy endpoint was the proportion of participants with <50 HIV-1 RNA copies/mL at week 48 (Food and Drug Administration snapshot approach; non-inferiority margin -10%). Of the 734 participants randomised, 728 were treated (364 per group) and included in the analyses.5
DRIVE-FORWARD is a randomised, controlled, double-blinded, multicentre, non-inferiority trial. Antiretroviral treatment-naïve adults (≥18 years) with ≥1000 HIV-1 RNA copies/mL were randomised (1:1) to once-daily DOR at 100 mg, or darunavir 800 mg plus ritonavir 100 mg (DRV/r) once daily with two investigator-selected NRTIs (tenofovir and emtricitabine, or abacavir and lamivudine) for up to 96 weeks.8
The primary efficacy endpoint was the proportion of participants with <50 HIV-1 RNA copies/mL at week 48 (Food and Drug Administration snapshot approach; non-inferiority margin -10%). Of the 769 participants randomised, 766 were treated (383 per group) and included in the analyses.7
Change in Fasting Lipids: DRIVE-AHEAD Week 192
Change in fasting lipids (mg/dL)
Participants who continued DOR/3TC/TDF maintained a favourable lipid profile, showing minimal change in all lipid measures
Participants who switched from EFV/FTC/TDF had substantial reductions in LDL-C, non HDL-C, TC and triglycerides
TC:HDL-C ratio showed minimal change in both groups: 0.15 and 0.22, respectively
Data from week 192 of the DRIVE-AHEAD trial evaluating durability in participants who entered a 96 week study extension and received open-label DOR/3TC/TDF
Continued DOR/3TC/TDF
Switched to DOR/3TC/TDF
Figures adapted from Orkin C et al. 2021.9
Change in Fasting Lipids: DRIVE-FORWARD Week 192
Change in fasting lipids (mg/dL)
Participants who continued DOR + 2 NRTIs maintained a favourable lipid profile, with minimal changes in all lipid measures
Participants who switched from DRV/r + 2 NRTIs had substantial reductions in LDL-C, non-HDL-C, TC and triglycerides
There were only minimal changes in the TC:HDL-C ratio for participants who continued DOR + 2 NRTIs and those who switched to DOR + 2 NRTIs (−0.2 and −0.4, respectively)
Data from week 192 of the DRIVE-FORWARD trial evaluating durability in participants who entered an open-label 96-week extension phase and either continued to receive DOR+2NRTIS or switched from DRV/r+2NRTIs to DOR+2NRTIs at week 96
Continued DOR + 2 NRTIs
Switched to DOR + NRTIs
Figures adapted from Cahn P et al. 2021.10
DRIVE SHIFT 144 Week Weight Change Data
Participants in the DRIVE SHIFT study switched from a baseline regimen consisting of 2 NRTIs in combination with a PI plus either ritonavir or cobicistat, or elvitegravir plus cobicistat, or an NNRTI to DELSTRIGO (doravirine/3TC/TDF).11
Primary efficacy endpoint
The proportion of participants with HIV-1 RNA <50 copies/ml at Week 48 in the immediate switch group compared to Week 24 in the delayed switch group.11
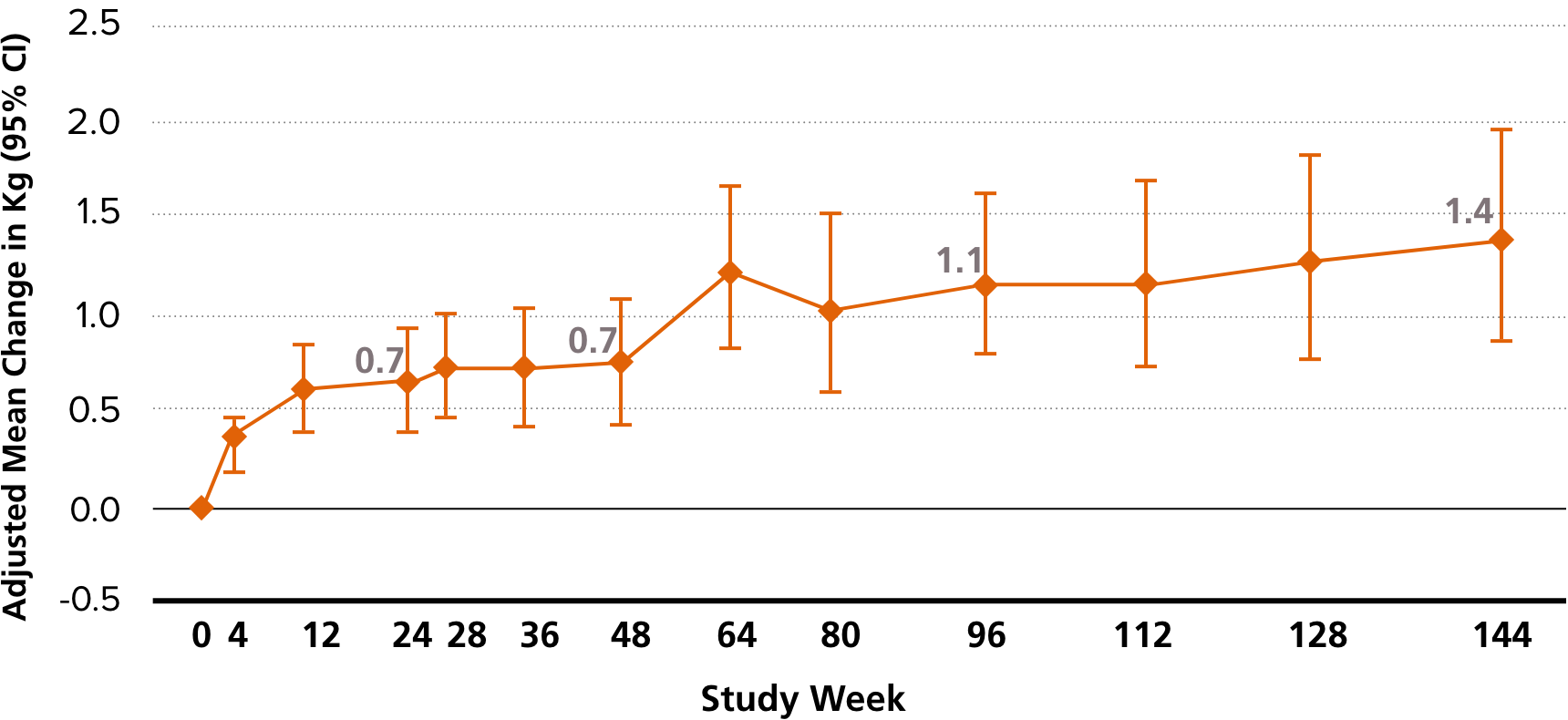
Findings: modest weight gain after more than 2 years on doravirine/3TC/TDF which would be no higher than that expected in an otherwise healthy population.12
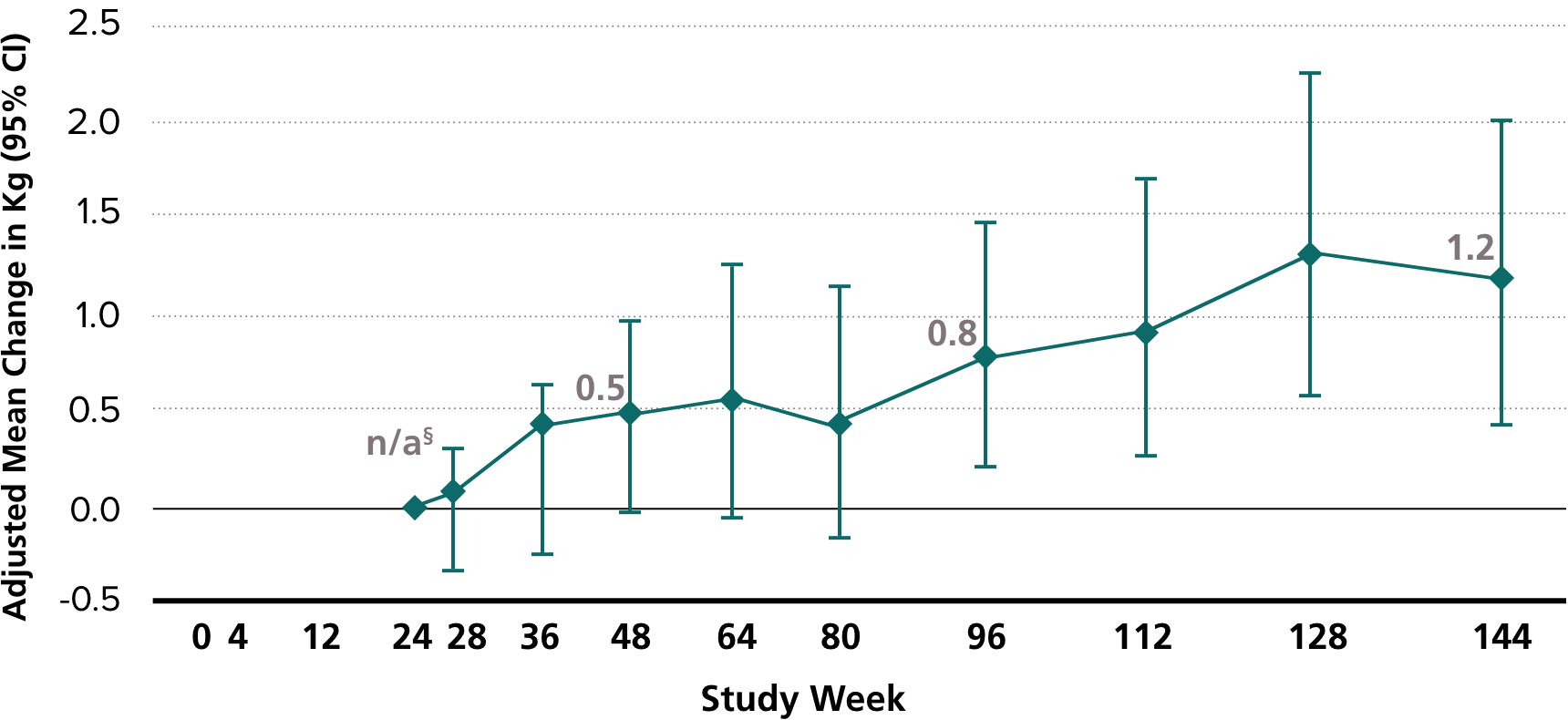
The adjusted mean weight gain was 1.4 kg at ~ 2.8 years after switch in the immediate switch group and 1.2 kg at ~ 2.3 years after switch in the delayed switch group.12
Study group = immediate switch group (n=438)
Study group = delayed switch group (n=209)
Adapted from Kumar P et al. 2021.12
†Adjusted for weight at time of switch, race (Black/non-Black), ethnicity (Hispanic/other), sex, age, prior therapy class, baseline CD4+ T-cell count, and baseline HIV-1 RNA.
§Delayed switch group switched to doravirine/3TC/TDF at Week 24.
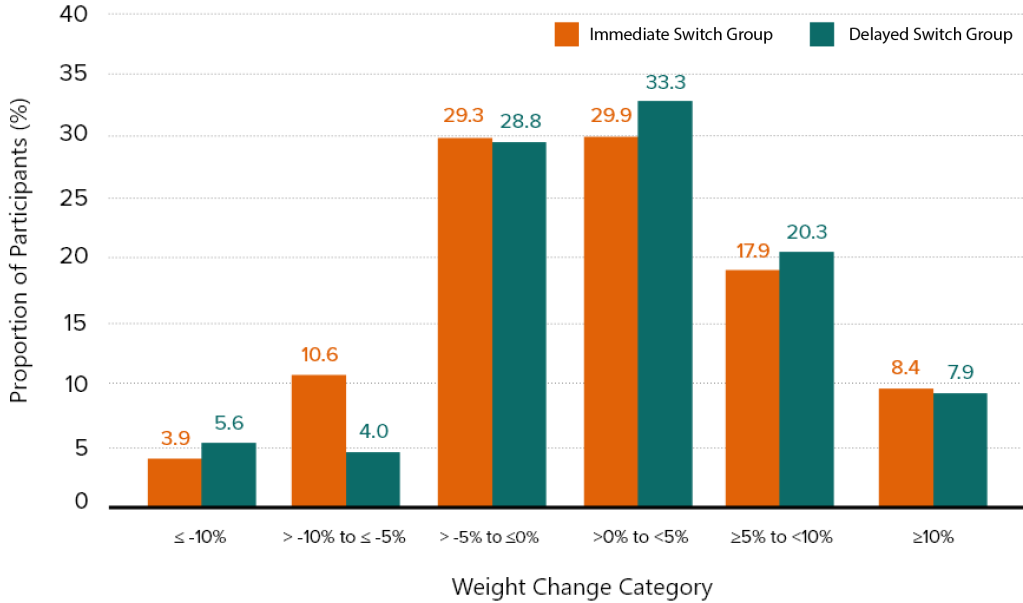
Adapted from Kumar P et al. 2021.12
From time of switch to Week 144.12 ~70% gained less than 5%, ~20% gained 5-10%, and ~8% gained 10% or more
4 Years of Experience from DRIVE-FORWARD and DRIVE-AHEAD Trials: Weight Change from Baseline13
Change in Body Weight: DRIVE-FORWARD / DRIVE-AHEAD Week 192
Median weight gain from baseline to Week 192 was low (~2 kg) in both trials
Figure adapted from Molina JM et al. 2021.13
aNRTIs were TDF/FTC (87% of participants) or Abacavir/3TC (13% of participants); Error bars indicate Q1 and Q3 for weight change.
Alberti KGMM et al., Circulation, 2009;120:1640-1645.
Castaneda A et al., World J Diabetes, 2018;9:66-71.
Collins LF et al., Metabolic Syndrome in HIV/HCV Co-infected Patients, Curr Treat Options Infect Dis. 2019 December ; 11(4): 351–371. doi:10.1007/s40506-019-00207-3.
Gooden, T.E et al., 2021, Incidence of cardiometabolic diseases in people with and without human immunodeficiency virus in the United Kingdom: A population-based matched Cohort Study, The Journal of Infectious Diseases, 225(8), pp. 1348-1356. Available at: https://doi.org/10.1093/infdis/jiab420.
Orkin C, Squires KE, Molina JM, et al.; and DRIVE-AHEAD Study Group. Doravirine/lamivudine/ tenofovir disoproxil fumarate is non-inferior to efavirenz/emtricitabine/tenofovir disoproxil fumarate in treatment-naive adults with human immunodeficiency virus–1 infection: week 48 results of the DRIVE-AHEAD trial. Clinical Infectious Disease. 2019;68(4):535–544.
Orkin C et al. Doravirine/lamivudine/tenofovir disoproxil fumarate (TDF) versus efavirenz/emtricitabine/TDF in treatment-naïve adults with Human Immunodeficiency Virus type 1 infection: week 96 results of the randomised, double blind, phase 3 DRIVE-AHEAD non-inferiority. Clinical Infectious Disease. 2020: 1–10.
Molina JM, Squires K, Sax PE, et al.; for the DRIVE-FORWARD Study Group. Doravirine versus ritonavir-boosted darunavir in antiretroviral-naive adults with HIV-1 (DRIVE-FORWARD): 48-week results of a randomised, double-blind, phase 3, non-inferiority trial. Lancet HIV. 2018;5(5): e211–e220. doi:10.1016/S2352-3018(18)30021-3. Epub. 2018 March 25.
Molina JM et al. Doravirine versus ritonavir-boosted darunavir in antiretroviral-naïve adults with HIV-1 (DRIVE-FORWARD): 96 week results of a randomised, double-blind, non-inferiority, phase 3 trial. Lancet HIV. 2020;7:16–26.
Orkin C et al., The safety and efficacy of maintenance with doravirine/lamivudine/tenofovir through 192 weeks in adults with HIV-1: Results from the DRIVE-AHEAD clinical trial. Poster presented at the International AIDS society meeting, July 18-21, 2021.
Cahn P et al., The efficacy and safety of maintenance with doravirine plus two NRTIs after initial suppression in adults with HIV-1 in the DRIVE-FORWARD clinical trial: Results from the study extension through 192 weeks. Poster presented at ID week 2021, September 29-October 3, 2021.
Johnson M et al. Switching to doravirine/lamivudine/tenofovir disoproxil fumarate (DOR/3TC/ TDF) maintains HIV-1 virologic suppression through 48 weeks: results of the DRIVE-SHIFT trial. J Acquir Immune Defic Syndr. 2019;81(4):463–472.
Kumar P et al. Switching to Doravirine/Lamivudine/Tenofovir Disoproxil Fumarate (DOR/3TC/TDF) Maintains HIV-1 Virologic Suppression Through Week 144 in the DRIVE-SHIFT Trial. J Acquir Immune Defic Syndr. 2021 Feb 17. doi: 10.1097/QAI.0000000000002642. Epub ahead of print.
Molina JM et al., Safety and Efficacy of doravirine in Treatment-Naive Adults with HIV-1: 4 Years of Experience from the DRIVE-FORWARD and DRIVE-AHEAD Clinical Trials. Poster presented at the 18th European AIDS Conference (EACS), October 27-30, 2021.
This section of the website contains promotional information intended for UK Healthcare Professionals only. If you are not a UK healthcare professional, please click here. GB‑NON‑10777 | Date of Preparation: January 2025
Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to Merck Sharp & Dohme (UK) Limited (Tel:0208 154 8000)